
Twelve principles to guide treatment of Crohn's disease

We have many new drugs to manage Crohn’s disease.
This is great for clinicians and patients alike.
But it can be overwhelming, and not all drugs are available to all patients across the world. Restrictions apply: cost, guidelines, approvals, insurance providers to name just a few.
Follow this set of simple principles to guide care whatever the therapy.
1/ Crohn's disease is progressive
With long-term, irreversible bowel damage, disability and poor quality of life the result.
2/ Diagnostic delay is associated with worse outcomes
Ensure effective systems are in place to mitigate against this.
3/ Disease complications can be prevented with effective therapy
This may involve over-treating a few patients to avoid under-treatment the majority.
4/ Starting effective therapy early results in best outcomes
Effective therapy means an advanced therapy -
anti-TNF or
anti-p40 or
anti-p19 or
anti-integrin or
a JAK inhibitor and
combination therapy (in the future)

5/ There is a disconnect between symptoms and inflammation
Use non-invasive monitoring tools like faecal calprotectin and intestinal ultrasound.
6/ Biosimilar anti-TNFs are the most cost effective drugs
They work, are accessible, and allow for rapid dose escalation.
This might be
infliximab plus azathioprine or
adalimumab (plus or minus azathioprine) and
ustekinumab (available across Europe July 2024)
7/ Early ileo-caecal resection should be offered to patients
And it offers excellent long-term outcomes for many.
This should be offered to all newly diagnosed patients with limited terminal ileal disease.
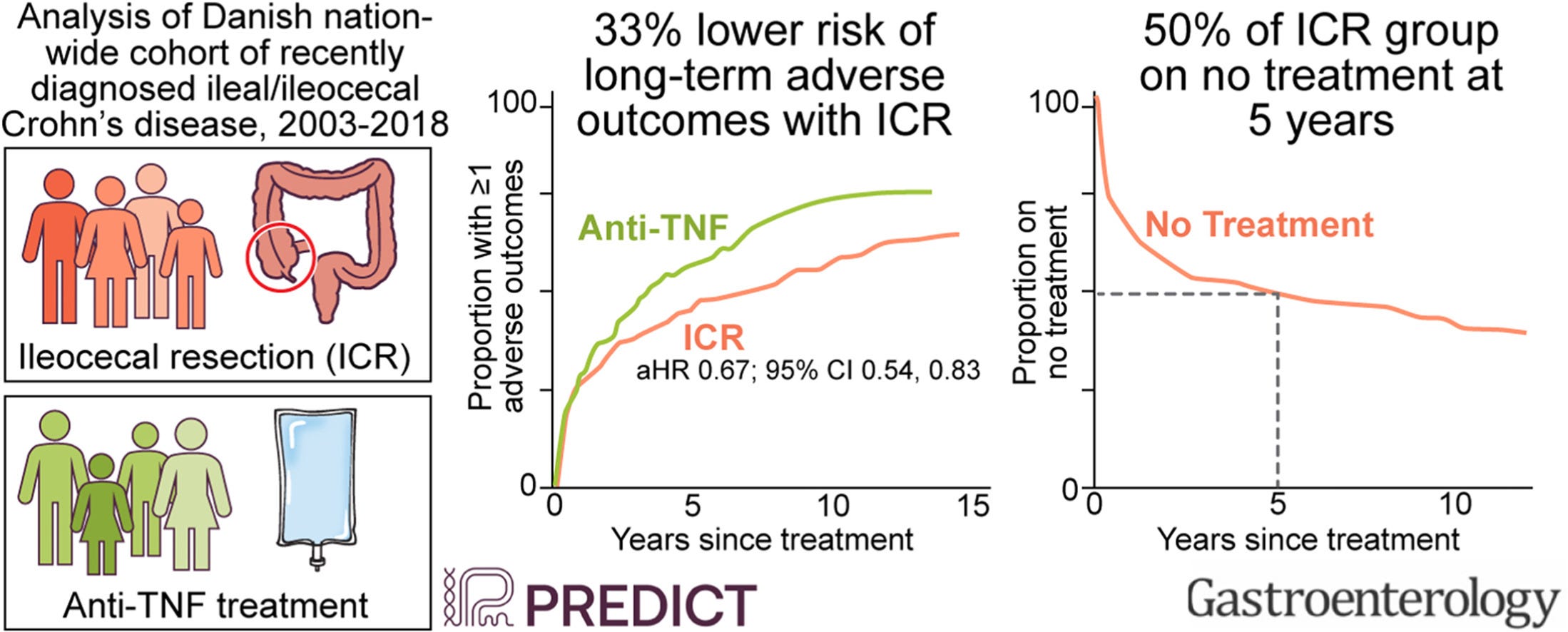
Ensure good systems in place to monitor for recurrence with prophylactic therapy in at risk patients.
8/ 5-ASA compounds do not work effectively in Crohn's disease
They only work at the mucosal level and Crohn's is a transmural disease.
Do not use 5-ASA in Crohn’s disease.
9/ Steroids do not heal the mucosa in Crohn's disease
Do not (over)use them.
10/ Dietary therapy is important in Crohn's disease
Use exclusive enteral nutrition in place of steroids for small bowel disease.
It works in adults as well as kids.
Use low residue diet for stricturing disease.
Mediterranean diet for everyone else.
11/ The psychological harm associated with Crohn's disease is high
It starts early in the disease course and includes suicidal ideation and completed suicide.
Do not underestimate this.
12/ Work as a multi-disciplinary team
And put the patient at the centre of that team.
The cornerstone of any good IBD team are IBD specialist nurses.
Other members of an effective IBD MDT:
surgeons
dieticians
radiologists
pathologists
pharmacists
psychologists
research team
administrative team
rheumatologists, dermatologists and ophthalmologists
With your team focus on patient centered care and try to think holistically.
Point 7 is very interesting to me as someone who didn't receive a crohn's diagosis until AFTER I'd had an ileo-caecal resection. Even though it doesn't quite fit my case, it seems about as close as I can get. I've struggled to find any studies/outcomes on people whose Crohn's was only diagnosed via ICR histology (and I had no Crohn's symptoms for the first 50 years of my life - go figure... they assumed they were removing a cancer) - even though the one time I saw an IBD consultant, he tried to tell me my case wasn't that uncommon.